5 things we learned about changing behaviors for antibiotic stewardship


What is needed to better harness the huge potential of behavior change science for antibiotic stewardship? This is the question we set out to answer last year.
o look into the potential of behavior change science, we tried our hand at some human-centered design(opens in a new tab) and proved our number one hypothesis—that this is a tricky field to tackle.
We should say from the outset that our project didn’t generate the innovative ideas we hoped for, but it was a valuable learning experience. Here are five things we learned that could help future initiatives to have more impact.
1. The interchangeable use of ‘awareness’ and ‘behavior change’ is harming progress
Awareness of an issue is not enough to change people’s behavior. Yet, when it comes to antibiotic stewardship interventions, the lines between the two are often blurred.
Campaigns that rely on awareness alone fail to support responsible drug-seeking and prescribing practices in a sustainable way. This undermines the potential of behavioral science.
The partnership between the behavioral Insights Team(opens in a new tab) and Public Health England(opens in a new tab) is a great example of truly looking at antibiotic stewardship through a behavioral lens. Their 2015 review of resistance-driving behaviors led to the trial of social norm feedback(opens in a new tab) to improve antibiotic prescription practices by GPs in the UK—this showed potential for sustained impact(opens in a new tab).
2. Human-focused research is vital to create effective and accepted tools
behavioral research should not only be tested with people but co-created with them. By embracing a human-focused perspective from development to implementation, we can more accurately identify key behaviors and levers for change, all while gaining validation and support from target communities.
Our human-centered design project showed first-hand how understanding prescribers and patients—the decision-makers and end-users—can pinpoint opportunities for change in antibiotic use. For example, by mapping patient care journeys we noticed key moments at which a behavioral intervention could improve prescribing practices while also supporting good care.
But we didn’t spend enough time understanding the context. The project focused on digital interventions that, while helpful, were not scalable in those countries. Aligning with new technology is a good tactic, but only by understanding people in their communities can we develop appropriate, accepted and effective behavioral approaches.
3. Start with ‘gatekeepers’ to understand the big picture
Antimicrobial ‘gatekeepers’ include all those who provide antibiotics: doctors, pharmacists, community healthcare workers and alternative caregivers. Their names and responsibilities vary across countries and health systems.
Starting with everyone in this group provides a holistic understanding of how antibiotics are prescribed and sold in the community. These big picture insights help to hone in on the most suitable targets and approaches for intervention.
Heading into our project we hoped to develop interventions focused on retail pharmacists. We scoped some interesting concepts that tried to sidestep financial drivers to provide antibiotics through encouraging customer loyalty based on good care, not prescriptions.
But we struggled to tap into this sector successfully. Looking at the wider ‘gatekeeper’ base we saw that GPs were most ready and willing to change, given the right tools—so this group became our target.
4. Generalising can help us create rapid, widespread change
As behaviors are context-specific, the most effective behavior change approaches are tailored to audiences and their setting. But we must be prepared to generalize to some extent, given the infinite number of contexts globally where antibiotic stewardship initiatives would be useful.
Identifying similarities and differences between settings allows us to share and repurpose existing evidence, rather than starting from scratch.
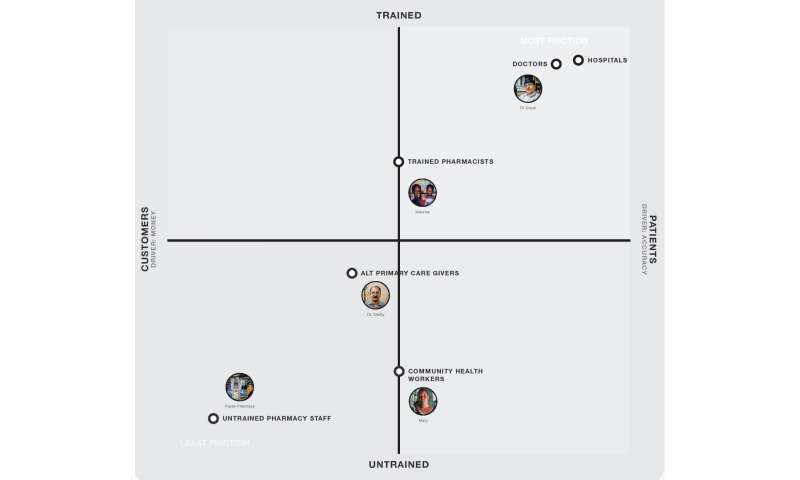
For example, by talking to ‘gatekeepers’ in India and Kenya (pictured below) we found common characteristics that drove prescription practices: level of training and whether they perceived antibiotic consumers as patients or customers.
Recognising common characteristics across different contexts helps scale ideas. This is vital to create change more widely. Critical to this is deciding what is ‘good enough’ and appreciating that waiting for a perfect or permanent solution will not help us advance antibiotic stewardship quickly.
5. We need to join up research and implementation
There is already a significant body of research demonstrating effective behavior change interventions for antibiotic stewardship. Often, this research is based on strong randomized control trial data.
But this work has too rarely made it through to practice in real-world settings. Barriers span the translation, approval, launch and embedding of behavior change programs into healthcare systems in a sustainable way.
There are few institutions with the capability to support the translation process. This gap must be addressed if we are to realize the potential of behavioral approaches.
- Case study: human-centered design for antibiotic stewardship in Kenya and India
- The first step in the project was to review existing behavioral research. Based on this, our hypothesis was that a far greater impact on antibiotic prescribing practice could be achieved if more accessible, adaptable, and evidence-based tools could have an impact on antibiotic prescribing practices.
- We chose human-centered design(opens in a new tab) to develop prototype tools. This is a creative method for problem-solving that works closely with people to co-create and iterate solutions that meet their needs.
- We commissioned a design agency to develop prototypes that could support frontline antibiotic ‘gatekeepers’ in middle-income countries to prescribe fewer unneeded antibiotics.
- The field work took place in Bangalore, India, and Nairobi, Kenya. We talked to patients, pharmacists and other healthcare professionals to understand how antibiotics were used and viewed, and to identify opportunities where design could influence stewardship behaviors.
- We came up with ideas targeting different antibiotic ‘gatekeepers’. Tools specifically for general practitioners (GPs) were taken forward for development and testing.
- A digital tool called SmartPrescriptions was prototyped. This simple Electronic Medical Record platform allows doctors to input patient symptoms, diagnosis and their prescription. The tool provides quick access to prescribing guidelines relevant to the information entered. It flags when a prescription for antibiotics does not match the recommended treatment. It is also a communication tool—doctors can fill in the record together with the patient to help explain the prescription. They can send follow-up text messages to continue care even when no medication is prescribed.
- This tool was evaluated through a small set of user-assisted tests. No randomized control trial was held.
- Through evaluation, we found the project approach had benefits, but the final tool was not sufficiently novel or in line with original objectives to be advanced.
Source: Read Full Article
Related posts:
 We Answer All Your Burning Questions About Deodorant
We Answer All Your Burning Questions About Deodorant
 5 Things Your Vagina Can Tell You About Your Health
5 Things Your Vagina Can Tell You About Your Health
 I Finally Met My Birth Mother — And Learned About My Family History of Endometriosis
I Finally Met My Birth Mother — And Learned About My Family History of Endometriosis
 How one writer changed the way we talk about mental health
How one writer changed the way we talk about mental health
 Making Halloween Less Scary for Teens With Allergies, Asthma
Making Halloween Less Scary for Teens With Allergies, Asthma