Monitoring CO2 to assess risk of indoor airborne SARS-CoV-2 transmission
Amid the coronavirus disease (COVID-19), caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), scientists aim to determine ways to limit viral transmission, particularly in indoor spaces.
The risk of infection with SARS-CoV-2 increases in indoor spaces without proper ventilation. That is why public health officials recommend the use of masks in indoor spaces. A new guideline for mitigating the indoor airborne transmission of SARS-CoV-2 also recommends limiting the time spent in a shared space with an infected person.
Researchers at the Department of Chemical Engineering, Massachusetts Institute of Technology, revealed that the SARS-CoV-2 transmission risk depends on both the pathogen concentration and exposure time.
In the study, which appeared on the pre-print server medRxiv*, the team developed a general mathematical theory to predict airborne transmission risk from carbon dioxide (CO2) time series in real-time and clarify different estimates that steer the guideline. The study findings were based on the assessment of transmission risk and implementing the guideline by CO2 monitoring in university classrooms and office spaces.
Carbon dioxide and airborne disease transmission
The SARS-CoV-2 spreads primarily via respiratory droplets when in close contact with an infected person. There is overwhelming evidence that the virus can also spread through exhaled aerosol droplets suspended in indoor air.
Scientists believe that airborne transmission explains “super-spreading events,” which caused skyrocketing cases in many countries. The dominance of indoor airborne transmission is supported by the fact that face mask orders were more effective in limiting COVID-19 spread than social distancing orders or lockdowns.
A recent study of viral spread at Massachusetts public schools where face-mask orders were implemented found no significant effect of social distance orders, ranging from 3 feet to 6 feet.
Lastly, studies have also demonstrated the detection of infected virions suspended in hospital room air as far as 18 feet from an infected patient. This provides direct evidence that the virus thrives in the air and spread through infected aerosols.
For decades, carbon dioxide measurements have been used to quantify airflow and zonal mixing in buildings to guide the design of cooling, heating, and ventilation systems.
High CO2 levels indoors are tied to poor health. Reports have also shown the link between CO2 levels and the concentration of airborne bacteria in schools. At the same time, correlations between outdoor air exchange rates and respiratory infections in dormitories have also been reported.
Measuring CO2 levels
In the current study, the team developed a safety guideline for mitigating the indoor airborne transmission of SARS-CoV-2 in terms of CO2 concentration. This way, it will be apparent that aside from limiting CO2 concentration, they should also limit occupancy time.
The team’s mathematical model demonstrates the effects of pathogen filtration, sedimentation, and deactivation, apart from the aerosol production rates, which alter the relative concentrations of airborne pathogen and CO2.
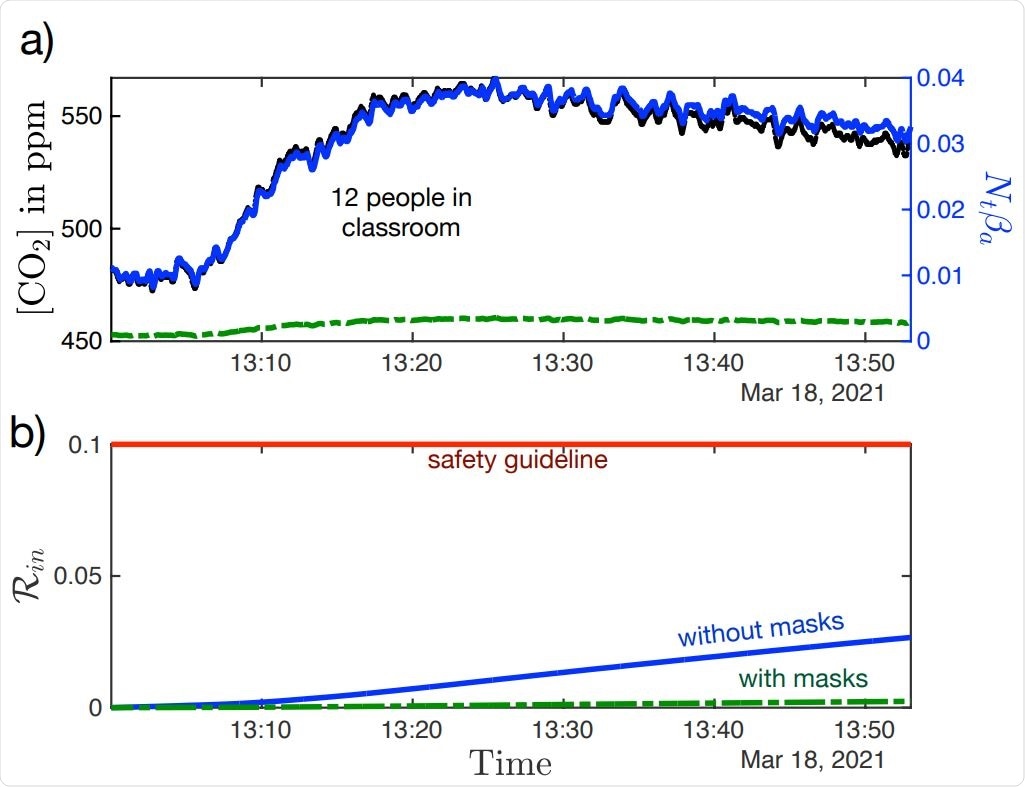
The new guideline recommends limiting transmission by wearing face masks, filtrating air, and imposing quiet spaces. The team also rephrased the guideline in terms of CO2 concentration. They modeled the illness transmission dynamics, allowing for the risk of indoor airborne transmission to be evaluated from CO2 measurements obtained in real-time.
The researchers applied the model in office and classroom settings. These demonstrate how CO2 monitoring, alongside safety guidelines, can help control the spread of COVID-19 in indoor spaces. The guideline does not only apply to SARS-CoV-2 but also a wide range of respiratory infections.
The simple guideline and the mathematical formula linking CO2 data to transmission risk allowed for the real-time assessment of transmission risk in indoor spaces.
“Our transmission theory and safety guideline provide a quantitative basis for the use of CO2 monitors in assessing the risk of indoor airborne disease transmission of indoor airborne disease transmission,” the team noted in the study.
The study results also allow for building-scale optimization of public health using CO2 sensors. The model also provides a blueprint for using CO2 monitors to control the spread of SARS-CoV-2 in indoor and shared spaces. Apart from COVID-19, the method and sensors can track other viral infections, such as seasonal flu.
*Important Notice
medRxiv publishes preliminary scientific reports that are not peer-reviewed and, therefore, should not be regarded as conclusive, guide clinical practice/health-related behavior, or treated as established information.
- Bazant, M., Kodio, O., Cohen, A., Khan, K., Gu, Z,, and Bush, J. (2021). Monitoring carbon dioxide to quantify the risk of indoor airborne transmission of COVID-19. medRxiv. https://www.medrxiv.org/content/10.1101/2021.04.04.21254903v1
Posted in: Medical Research News | Disease/Infection News
Tags: Bacteria, Coronavirus, Coronavirus Disease COVID-19, Flu, Hospital, Pathogen, Public Health, Respiratory, SARS, SARS-CoV-2, Severe Acute Respiratory, Severe Acute Respiratory Syndrome, students, Syndrome, Virus

Written by
Angela Betsaida B. Laguipo
Angela is a nurse by profession and a writer by heart. She graduated with honors (Cum Laude) for her Bachelor of Nursing degree at the University of Baguio, Philippines. She is currently completing her Master's Degree where she specialized in Maternal and Child Nursing and worked as a clinical instructor and educator in the School of Nursing at the University of Baguio.
Source: Read Full Article
Related posts:
 Does climate play a large role in SARS-CoV-2 transmission?
Does climate play a large role in SARS-CoV-2 transmission?
 Neutralizing antibodies to SARS-CoV-2 in mice depend on Fc effector function
Neutralizing antibodies to SARS-CoV-2 in mice depend on Fc effector function
 GSK-3 inhibitors show promise in treating coronavirus infections
GSK-3 inhibitors show promise in treating coronavirus infections
 Researchers develop assay for qualitative assessment of SARS-CoV-2 neutralizing antibodies
Researchers develop assay for qualitative assessment of SARS-CoV-2 neutralizing antibodies
 Researchers evaluate antibodies that inhibit SARS-CoV-2 RBD variants with a novel assay
Researchers evaluate antibodies that inhibit SARS-CoV-2 RBD variants with a novel assay