Young women who suffer a heart attack have worse outcomes than men

Women aged 50 or younger who suffer a heart attack are more likely than men to die over the following 11 years, according to a new study published today (Wednesday) in the European Heart Journal.
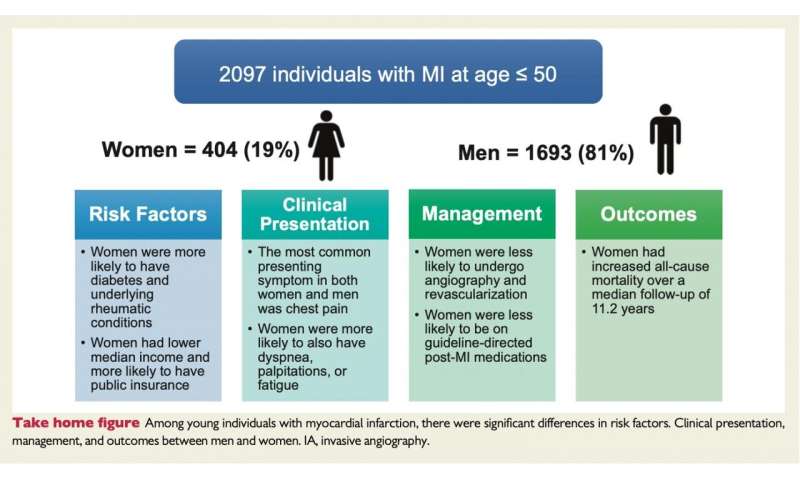
The study found that compared to men, women were less likely to undergo therapeutic invasive procedures after admission to hospital with a heart attack or to be treated with certain medical therapies upon discharge, such as aspirin, beta-blockers, ACE inhibitors and statins.
The researchers, led by Ron Blankstein, professor of medicine at Harvard Medical School and a preventive cardiologist at Brigham and Women’s Hospital, Boston, U.S., found no statistically significant differences between men and women for deaths while in hospital, or from heart-related deaths during an average of more than 11 years’ follow-up. However, women had a 1.6-fold increased risk of dying from other causes during the follow-up period.
Prof. Blankstein said: “It’s important to note that overall most heart attacks in people under the age of 50 occur in men. Only 19% of the people in this study were women. However, women who experience a heart attack at a young age often present with similar symptoms as men, are more likely to have diabetes, have lower socioeconomic status and ultimately are more likely to die in the longer term.”
The researchers looked at 404 women and 1693 men who had a first heart attack (a myocardial infarction) between 2000 and 2016 and were treated at the Brigham and Women’s Hospital and Massachusetts General Hospital in the US. During a myocardial infarction the blood supply to the heart is blocked suddenly, usually by a clot, and the lack of blood can seriously damage the heart muscle. Treatments can include coronary angiography, in which a catheter is inserted into a blood vessel to inject dye so that an X-ray image can show if any blood vessels are narrowed or blocked, and coronary revascularisation, in which blood flow is restored by inserting a stent to keep the blood vessel open or by bypassing the blocked segment with surgery.
The median (average) age was 45 and 53% (1121) had ST-elevation myocardial infarction (STEMI), a type of heart attack where there is a long interruption to the blood supply caused by a total blockage of the coronary artery. Despite being a similar age, women were less likely than men to have STEMI (46.3% versus 55.2%), but more likely to have non-obstructive coronary disease. The most common symptom for both sexes was chest pain, which occurred in nearly 90% of patients, but women were more likely to have other symptoms as well, such as difficulty breathing, palpitations and fatigue.
Prof. Blankstein said: “Among patients who survived to hospital discharge, there was no significant difference in deaths from cardiovascular problems between men and women. Cardiovascular deaths occurred in 73 men and 21 women, 4.4% versus 5.3% respectively, over a median follow-up time of 11.2 years. However, when excluding deaths that occurred in hospital, there were 157 deaths in men and 54 death in women from all causes during the follow-up period: 9.5% versus 13.5% respectively, which is a significant difference, and a greater proportion of women died from causes other than cardiovascular problems, 8.4% versus 5.4% respectively, 30 women and 68 men. After adjusting for factors that could affect the results, this represents a 1.6-fold increased risk of death from any cause in women.”
Women were less likely to undergo invasive coronary angiography (93.5% versus 96.7%) or coronary vascularisation (82.1% versus 92.6%). They were less likely to be discharged with aspirin (92.2% versus 95%), beta-blockers (86.6% versus 90.3%), angiotensin-converting enzyme inhibitors (ACE inhibitors) or angiotensin receptor blockers (53.4% versus 63.7%) and statins (82.4% versus 88.4%).
The study is the first to examine outcomes following heart attack in young men and women over such a long follow-up period. It shows that even after adjusting for differences in risk factors and treatments, women are more likely to die from any cause in the longer term. The researchers are unsure why this could be. Despite finding no significant difference in the overall number of risk factors, they wonder whether some factors, such as smoking, diabetes and psychosocial risk factors might have stronger adverse effects on women than on men, which overcome the protective effect of the estrogen hormone in women.
Prof. Blankstein added: “As fewer women had STEMI and more had non-obstructive myocardial infarction, they are less likely to undergo coronary revascularisation or to be given medications such as dual anti-platelet therapy, which is essential after invasive heart procedures. Also, the absence of obstructive coronary artery disease may raise uncertainty regarding the diagnosis and whether such individuals truly had a myocardial infarction or have elevated enzymes due to other causes.
“While further studies will be required to evaluate the underlying reasons for these differences, clinicians need to evaluate and, if possible treat, all modifiable risk factors that may affect deaths from both cardiovascular and non-cardiovascular events. This could lead to improved prevention, ideally before, but in some cases, after a heart attack. We plan further research to assess underlying sex-specific risk factors that may account for the higher risk to women in this group, and which may help us understand why they had a heart attack at a young age.”
In an accompanying editorial, Dr. Marysia Tweet, assistant professor of medicine at the Mayo Clinic College of Medicine and Science, Minnesota, U.S., writes that “it is essential to aggressively address traditional cardiovascular risk factors in young AMI [acute myocardial infarction] patients, especially among young women with AMI and a high burden of comorbidities. Assessing clinical risk and implementing primary prevention is imperative, and non-traditional risk factors require attention, although not always addressed”. Examples include a history of pre-eclampsia, gestational diabetes and ovary removal and she points out that depression was twice as common among women in this study compared to men; “young women with depression are six times more likely to have coronary heart disease than women without depression.”
She concludes: “This study . . . demonstrates the continued need—and obligation—to study and improve the incidence and mortality trajectory of cardiovascular disease in the young, especially women. We can each work towards this goal by increasing awareness of heart disease and ‘heart healthy’ lifestyles within our communities; engaging with local policy makers, promoting primary or secondary prevention efforts within our clinical practices; designing studies that account for sex differences; facilitating recruitment of women into clinical trials; requesting sex-based data when reviewing manuscripts; and reporting sex differences in published research.”
Source: Read Full Article
Related posts:
 Around half a million men who have sex with men in the EU need PrEP but cannot access it
Around half a million men who have sex with men in the EU need PrEP but cannot access it
 People who suffer maltreatment in childhood have a higher chance of multi-morbidity in later life
People who suffer maltreatment in childhood have a higher chance of multi-morbidity in later life
 Female Heart Attack Patients Fare Better If ER Doc Is a Woman
Female Heart Attack Patients Fare Better If ER Doc Is a Woman
 Shiatsu massage can help induce sleep for people who suffer a concussion, study shows
Shiatsu massage can help induce sleep for people who suffer a concussion, study shows
 80 per cent of men would rather be ill than admit to a problem
80 per cent of men would rather be ill than admit to a problem