Get cliterate: how a Melbourne doctor is redefining female sexuality

You can trace Professor Helen O'Connell's discovery of the full clitoris – and the rewriting of the world's anatomy texts – to two books: one that angered her and another that inspired. The first book, Last's Anatomy, she couldn't seem to escape. The 1985 edition was the set text for her surgical exam and – to her "utter disbelief" as a classic overachiever – she failed the test three times. She calls this the "ridiculous book"; it had almost no mention of the clitoris, and certainly no illustrations, yet there were two pages on the penis. To top it off, aspects of female genitals were described as a "failure" of male genital formation (O'Connell still has the book, the word "failure" underlined in blue pen).
"I knew at some point," she says, "that I was going to have to tackle that."
She came across the second book – a University of Melbourne social scientist showed it to her – a few months after finally passing her surgical exam, in 1989. It was called A New View of a Woman's Body and was published by the US Federation of Feminist Women's Health Centres. It's full of detailed drawings of vulvas. For the clitoris chapter, the female researchers took off their pants and compared themselves with illustrations in respected anatomy texts. Then they masturbated, observed each other and took notes of the many parts of the internal and external clitoris that were changed by, or contributed to, sexual pleasure or orgasm. Young Helen O'Connell, aged 27, found it "really cool" and the women's observations – though not scientific – "valid".
When she first tells me about this book in her consulting rooms in The Royal Melbourne Hospital's private wing, it's obvious she's still fascinated by these women and the way they watched and mapped each other's sexual responses. "Amazing methodology!" she laughs. "Don't you think? Just. Amazing." In the book, the researchers said they had no access to dead bodies or dissection rooms, so had to partially rely on old anatomy texts. And that was a lightbulb moment for O'Connell: she had access to dead bodies and dissection rooms at the University of Melbourne, where she was studying her master's of medicine in women's health. "We just needed to do good science and work it out from the cadavers," she says. And that, really, is how Helen O'Connell came to change the world of female anatomy forever.
I find myself sitting in O'Connell's office because, rather strangely, of Netflix. A few months ago I was watching a series called Explained, a show that packages the modern world – The Stock Market, Designer DNA, Cryptocurrency – into snappy 15- to 20-minute documentaries. On this particular night, the episode to load on my television was on the female orgasm. Around the eight-minute mark, the narrator said that in 1998 "the Australian urologist Helen O'Connell and her team discovered that the clitoris was way more powerful than we'd known". I sat up straight: a memory came flashing back to me.
It was 1998 and I was a young journalist at The Age, reading the day's news list. O'Connell had found that modern medical science was mistaken about the clitoris: the small button – or glans – that you can see is just the tip of the iceberg. Under the pubic bone, the organ looks like a wishbone with a body up to four centimetres long. Coming out of the body are legs, or crura, up to nine centimetres long, and also eggplant-shaped bulbs up to seven centimetres long. All these bits, O'Connell confirmed, are sensitive areas made of spongy tissue and become erect, just like the penis. A Melbourne doctor rewriting the anatomy books: this yarn, I thought, was a guaranteed front-pager.
But when I picked up the paper the next day, the lead front-page story was about a parasite that had shut down Sydney's water supply. Victorian premier Jeff Kennett was calling for states to have the power to veto potential hikes in the incoming GST, and visiting US Secretary of State Madeleine Albright had urged action on climate change. The clitoris story ended up on page six, squeezed between the paper's fold and a story about an American donation of wheat to Indonesia. Even in this, its moment of glory, the clitoris was treated as it had ever been: downgraded and difficult to find.
Sitting on my couch watching Netflix, it was O'Connell who fascinated me. It's been 20 years since that ground-breaking scientific paper: where was she now? What new mysteries of female sexuality had she solved? Had someone given this woman an Order of Australia? O'Connell's discovery was important for practical reasons: it gave surgeons a map of the key nerves, blood vessels and connecting parts of the clitoris so they could try to avoid destroying sexual sensitivity during any pelvic-area operation. O'Connell had witnessed many penis-related surgeries where great care was taken to avoid any loss of sexual function, but no one knew enough about the female anatomy to do the same for women.
Her work also inspired a generation of sex educators, therapists, artists and academics who use her research to answer some fundamental and persistent questions about sex. The clitoral v vaginal orgasm debate, the orgasm gap between heterosexual women and their male partners, small penises and "loose" vaginas, the so-called G-spot: all these things, sex therapists and researchers say, could be better understood if men and women knew more about the clitoris, and therefore female arousal. British writer Jessica Berens once said that without a proper map of the female bits, it's as if everyone's been driving around for ages and still not found where they want to go: a bit like Canberra. It's been 20 years since we've had a proper map, but are we, I wondered, there yet?

Helen O'Connell is not a sex guru. She is not Bettina Arndt or the eccentric sex therapist played by Barbra Streisand in the 2004 film "Meet the Fockers".Credit:Kristoffer Paulsen
I'm only three minutes late to meet O'Connell, but her medical secretary is phoning, checking my whereabouts. Every single minute is crucial to O'Connell, 56, because being a clitoris guru is just a sideline.
Australia's first female urologist, O'Connell is a surgeon who treats patients with lower urinary tract problems such as incontinence and obstruction. A gifted endoscopic surgeon, she fixes or removes things within the tiny spaces of the urinary tract using a small telescope. She's also Director of Surgery and Head of Urology at Western Health, a sprawling health network servicing 900,000 people in Melbourne's west. In her rather limited spare time – and for no payment – she chips away on her female anatomy research, publishing a paper only last year on her search for the elusive but famous G-spot. More on that later.
When I get up to her third-floor consulting rooms, O'Connell, assured and professional, welcomes me into her office. She's wearing a dark pants suit and cat's-eye maroon glasses, blonde hair to her shoulders. We start awkwardly: I thought the meeting was to merely discuss the prospect of a profile, but she's like, "I've got one hour now, begin!"
In one of her research papers – which, with a tangle of keys, she unlocks from a white cupboard – O'Connell details the history of the clitoris in anatomy. In the 16th century, Italian anatomist Realdo Colombo (who called it a "seat of lust") and his contemporary Gabriele Falloppio (he of Fallopian tubes fame) feuded over who found the clitoris first. Dutch anatomist Regnier de Graaf did a comprehensive job of describing it in the 17th century, even discussing the crucial clitoral bulbs. And in the 1840s, German anatomist Georg Kobelt published an extensive account of the female genitals, their spongy tissues, muscles, nerves and blood supply.
His black-ink drawings are like a landscape of rivers, lakes and tree roots. "Really beautiful," notes O'Connell, who says she simply used modern science to confirm much of his work.
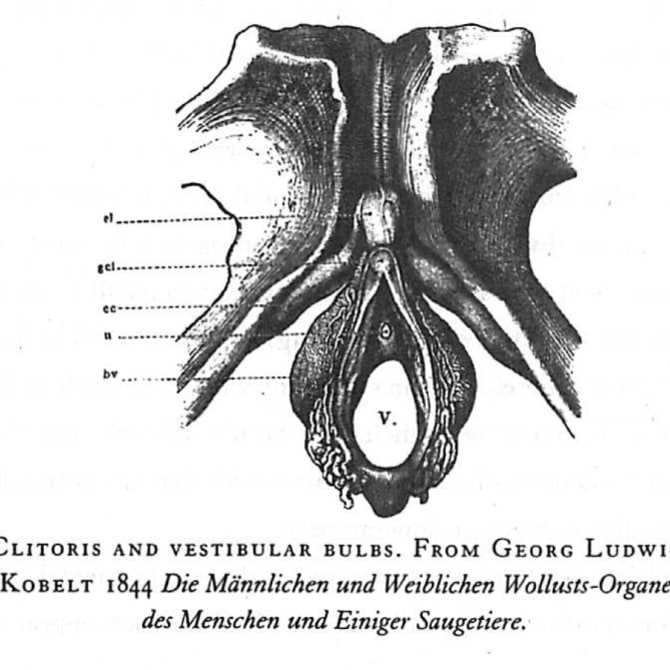
Helen O’Connell’s work built on the groundbreaking 1840s anatomy and “really beautiful” drawings of Georg Kobelt. Credit:Georg Ludwig Kobelt
But unlike O'Connell, Kobelt failed to connect all the internal bits as one structure, the clitoris, fed by the one nerve complex and blood supply. His work also left unexamined the relationship between the urethra, vagina and clitoris. Kobelt was soon forgotten anyway, as the clitoris fell out of fashion. That was the fault of Sigmund Freud, the bearded father of psychoanalysis, who declared in the early 1900s that clitoral orgasms were immature and "vaginal orgasms" mature. In 1948, the 25th edition of the seminal Gray's Anatomy removed the clitoris completely. While the clitoris made a comeback in later editions, only the part you can see – the glans – was noted.
O'Connell and her team took 10 cadavers and removed the pubic bone to expose the internal clitoris. They photographed what they saw and did laboratory tests on the tissues. At the time, anatomy texts often failed to mention the clitoral bulbs, which become engorged when aroused. Sometimes they were drawn half their size or put in the wrong place and were named "bulbs of the vestibule". A vestibule is a lobby or entrance hall, presumably to the vagina itself. "What the hell is the vestibule?" asks O'Connell, and we laugh, giving me the first glimpse of a lovely sense of humour behind the serious facade.
Anatomy books also connected the bulbs to the inner parts of the vulva. But O'Connell found this to be incorrect: they were joined to the clitoris body. Meanwhile, there was a whole bit of anatomy – the Bartholin's glands – that O'Connell couldn't find: they simply weren't where the anatomy books said. The standard texts also showed the clitoris flat against the pubic bone, but in reality, O'Connell found, it exists in three planes; with bits going everywhere. The 1995 edition of Gray's Anatomy said the clitoris's major nerve supply was "very small". But the nerves were actually "noticeably large", greater than two millimetres in width. O'Connell was "blown away" when she discovered how large they were. "There's a lot going on in those nerves," she says, with a smile.
In 2005, O'Connell confirmed her original research with magnetic resonance imaging (MRI) of 10 living women. "See just how amazingly bright it is?" she says. "It's because of the high blood flow." I'm holding this scientific paper and O'Connell is looking over my shoulder at a black-and-white scan of a healthy, non-aroused pelvic area. The clitoris stands out from the surrounding tissue in a white glow. She tells me she saw a patient's MRI today – a woman who was probably quite distressed – and there was little blood flow in that area. "It's as if there's no clitoris there. I've not tested this, but the tissue is probably very sensitive to stress levels."
O'Connell returns to her chair, leaving me with four papers to read later. I'm quite keen to read the one about the G-spot, but when I get home, I realise it's missing from the pile.

New York artist Sophia Wallace with her clitoris sculpture, Adamas
(Unconquerable).Credit:Sophia Wallace
New York artist Sophia Wallace is talking to me via Skype from her white-walled Brooklyn studio. When she picks up her laptop and shows me around it, I see a giant golden clitoris sculpture on a plinth. It's stylised, a little abstracted, but based on O'Connell's correct anatomy. "The shadow it makes is sort of like a penguin," she says, when I ask her to describe the shape. "It's like the inside of a very complex flower, maybe an orchid. But it is also robust and strong."
Since 2012, through her Cliteracy project and a popular TED Talk, Wallace has been evangelical about the true shape of the clitoris. She's written a human-dwarfing, giant wall of words called The 100 Natural Laws of Cliteracy, a sort a declaration of rights for the clitoris. Don't scoff: each year, an estimated three million young girls are at risk of having their external clitoris cut off, according to the World Health Organisation. One of the first laws Wallace wrote was a definition, which she holds up to me, big black letters on white card. And there, as part of that definition, is Helen O'Connell, the discoverer of the "precise anatomy, function, complexity and external and internal scale" of the clitoris.
Wallace despairs that, 20 years after O'Connell's research, the taboo around the clitoris persists and its true form remains unfamiliar. The Oxford Dictionaries still describe it as "a small, sensitive, erectile part of the female genitals at the anterior end of the vulva".
"I have to deal with censorship all the time," says Wallace. Her web-host hides pages and sections of her website, where you can buy an anatomically correct clitoris pendant or, for that special man in your life, "clitlink" cufflinks. Facebook and Instagram take down some posts. "I think we've come about five per cent of the way," says Wallace, when I ask her how "cliterate" society is now. "I continue to see these studies on what percentage of women orgasm through penetration or intercourse. And I am like, 'Who cares?' How many are giving pleasure and not getting pleasure? What are their barriers to pleasure? What is the clit's happy state? What does it have a right to expect? What is a good life for a clit?"
The sex education of young Helen O'Connell did not start well. The nuns at her Catholic girls' school told the 10-year-old to go home and ask her mother about sex. And so Mary O'Connell, who was deeply Catholic, took her daughter into the backyard of their middle-class home in Preston, in Melbourne's north. They stopped near the incinerator. "It was possibly the ugliest part of the backyard," remembers O'Connell. The man plants a seed in the woman, Mrs O'Connell told her confused daughter. "I had no idea what she was talking about," says O'Connell. "And Mum was just devastated with embarrassment about the whole thing." From that moment on, all further questions were directed to her older sisters. (O'Connell is the youngest of five, with three sisters, including twins, and a brother.)
Her father Kelvin, a public servant who worked in civil aviation, was "sort of a feminist", says O'Connell. "He never, ever indicated that you should not do something because you were female." Unusually for her era, Mary worked full-time as a bookkeeper by the time Helen was five. O'Connell remembers watching the moon landing in 1969 at school with a small group of kids whose mothers worked, while the other kids went home. "She would say, 'A woman's place is in the home,' but she was in the workplace, so I'm not sure how that worked. I think she thought she was expected to say that," O'Connell says. "But we all knew that Mum was happiest when she was working."
This was true for O'Connell, also, when it came to having kids of her own. With her first child, a son who is now 21, O'Connell had three weeks at home in a "blissful" state but felt "very strange at a profound personal level, an existential level". So she went back to her private practice, at first doing one session with patients a week. "I felt I knew who I was again. So the next week, I did two sessions." With her second child, a daughter who is now 20, she went back after two weeks. "It felt very strange to be full-time at home with healthy, perfect babies. I trained for 15 years to be a surgeon and none of that taught me how to be a mother." She pulled off being a top surgeon and a mother with "help, help, help": great husband help, office help, nannies. O'Connell also now has two adult step-children, but will go into no more details about her private life: "It's not a girls' magazine!"
At high school, O'Connell was popular. "My main memory as we walked through school," says Suzanne Barnes, one of O'Connell's best schoolmates, "is of everyone saying, 'Hi Helen, Hi Helen!' She knew everyone, was school captain and she had this personality that attracted people." She loved to party and, in medical school, was one of the lead singers in a rock band called Unfinished Business. She married the lead guitarist.
O'Connell had her heart set on being a surgeon, partly because her mother said she had good hands and that she must do something with them one day. And when she was two, she was operated on to fix a squint, which planted the idea that surgery could transform and cure. But why urology, which is essentially about what goes wrong in the wee department? She thought it had a great future. A senior surgeon had advised against general surgery; it was dead, he said. Turns out he was wrong. And O'Connell thought the urologists were well trained and she loved the range of surgery offered: through the urethra, into the bladder, kidney surgery, open abdominal and perineal.
Not everyone thought urology a good career move. Her mentor, Melbourne psychiatrist Lorraine Dennerstein, remembers a surgery interview panel asked O'Connell what sort of man would want to share their urinary problems with her (there were no female urologists in Australia at the time). "Well, we all laughed," says Dennerstein. "What sort of male wouldn't want to see her? She was young and attractive and some men prefer to share these intimate aspects with a woman doctor. And, anyway, many people with urinary problems were actually women. No one thought the women might be uncomfortable going to a male doctor." O'Connell does not remember this, but she does recall a male anaesthetist telling her she'd starve from lack of work. "I didn't say anything back; I just tucked it away and thought, 'I'm sure you are wrong.' "
O'Connell did not starve. She had no problem finding patients, male or female. Then in 1998, when the clitoris paper was published – the same year, coincidentally, that Viagra became available – a whole new world opened up. Her name is barely known in Australia – she's never received an OAM or anything like it – but she's regarded as an international clitoris guru; in 2007 the World Association for Sexual Health awarded her a gold medal, its highest honour.
O'Connell never talked about her research to her orthodox Catholic mother. But just before she died, in 1999, Mrs O'Connell watched an ABC television program about her daughter's discovery. "For all of her bizarre stuff with Catholicism," says O'Connell, suddenly crying behind her desk, "she was very proud."

Occupational therapist Anita
Brown-Major and her satin vulva puppet, which she uses in teaching.Credit:Eddie Jim
Occupational therapist Anita Brown-Major admits she might be the world's most embarrassing parent. She has three primary-school-aged daughters and gets around the inner-Melbourne suburb of Brunswick with a vulva puppet in her handbag. What's more, this red and pink satin puppet, which Brown-Major uses in her sexual health education work with the disabled, has a fully removable, anatomically correct clitoris based on O'Connell's research. "No one knows what the clitoris looks like, even though we had Helen's research so long ago," Brown-Major tells me over the phone. She also uses her puppet to train health professionals on basic genital anatomy. You might think health-sector workers wouldn't need to meet her satiny friend – but no. Brown-Major often gives her classes some plasticine and asks them to construct a model of female erectile tissue.
I said, 'All right boys, you can draw a dick and balls, but can you draw a clitoris?'
"Everyone does a little ball and puts it in the middle of the table," she says. In a recent class, only two of the 30 health professionals actually made the correct version. The other day the Brown-Majors had friends over, a family of four boys. One of the boys took to drawing a penis and testicles all over the place. "I said, 'All right boys, you can draw a dick and balls, but can you draw a clitoris?' It stopped them dead in their tracks. My daughters nearly died."
We're somewhere in the bowels of Footscray Hospital, the biggest in the Western Health network. We make seemingly random right-angled turns, sweep into lifts then out, and clip at a brisk pace down grey, windowless corridors. "You can see why Footscray needs an upgrade," says O'Connell. The state government has promised a $1.5 billion replacement.
I've managed to squeeze more time out of O'Connell, but plans to follow her around the hospital have gone awry. It wasn't in her diary and now it's 11am and she's got a million things to do. She had ward rounds at 7.15am, an educational session for trainees at 8am, and another meeting after that on complex patient problems. She's just had a meeting with someone about the correct sort of needle the hospital should order to inject Botox into the bladder. She's got a meeting soon with a senior doctor about his entitlements. So she can talk now, but only until – she looks at her watch – 11.50am.
We come to an office with a name plate announcing Helen O'Connell, Director of Surgery. Inside is a much more modest workspace than her private consulting rooms, which have views of a boulevard of trees. Here, the vista is the wall of the opposite hospital wing. On her desk is a white mug with a crescent of pink lipstick on its edge. We sit down at a small table near the window: O'Connell, myself and Western Health's media manager, Paula Wilson.
Running the department of surgery and urology unit of a major metropolitan health network is a long way from where O'Connell began as the only woman practising urology in Australia. Her first urology meetings were divided into functions for the urologists and a social program for their wives. She remembers, in 1991, a lunch function with a bikini parade, which she avoided. "I don't think they had anything like that ever again. The game was up." She reflects on those days as "lonely rather than particularly sexist"; she just got on with things.
An early mentor introduced her to Dr Edward McGuire, a hugely influential American urologist who developed key techniques in female urology and bladder science generally. In 1993, O'Connell flew to Houston, Texas, to meet McGuire and he agreed to take her on for a one-year advanced training fellowship. He taught O'Connell a minimally invasive technique to treat the common problem of stress incontinence, when movement, such as coughing or lifting things, puts pressure on the bladder and it leaks.
It involved making a sling of lower-abdomen tissue to restore support to the urethra, reducing the size of the surgical cut previously required as well as complications. O'Connell believed this method would become the most popular solution to stress incontinence, but it was soon overtaken by synthetic mesh slings, which were considered even less invasive and easier to recover from.
O'Connell was not keen on synthetic mesh: she believed it risky because the body could reject it, so she never used it on her patients. She would not say this herself – because she's too humble and worried about the trauma that has been caused – but, it turns out, she was correct in her judgment. Hundreds of thousands of women with mesh implants are problem-free but, in an unfolding medical debacle, thousands of Australian women have suffered the despair of debilitating pain, persistent infections and lost sex lives from failed mesh operations.
Since 2014, the Australian government has prohibited the use of many mesh products used for surgery for incontinence and pelvic organ prolapse. O'Connell has operated on about 100 women to remove the mesh and sits on various government and professional committees, trying to get a registry set up to track the quality of care. "It is sad the way things have evolved, but these problems need significant government support and cannot be rectified by the professions without it."
Anaesthetist Belinda Schramm, who has worked with O'Connell since 2002, says her friend goes the extra mile for her patients. "She sees a lot of female patients who have bounced from one specialist to the next, trying to find a solution, and Helen is very committed to them." Schramm says O'Connell is always there for advice and checks in with how everyone is, from the theatre nurses to technicians. She also likes to invite colleagues from the hospital for dinner. Schramm remembers one of O'Connell's dinners for 14 people, which included possibly the largest fish Schramm had ever seen. "She comes home from work and cooks like Nigella."
Schramm says O'Connell is incredibly focused as a surgeon but also, underneath, a free spirit. One night around 2008, Schramm says, they went dancing, "really bad, middle-aged-mum dancing". A young theatre technician had promised to take them out, but the venue was unexpectedly awful. "We ended up in a laneway where you had to dodge dumpsters to get in. The music was horrendous – probably rave, electronic, completely undanceable. But Helen, this professor of surgery, was out on the dance floor all night, having a fantastic time."
Dancing, tennis and long walks along the Yarra are the release valves of an incredibly driven person. I look at O'Connell's CV: a 32-page scroll of, among other things, accreditations, teaching positions and professional education, and I wonder what continues to drive her. She went into surgery because her mother said she had good hands, because she could see the transformative power of surgery. But where does the drive come from now, at 56?
Sitting next to the window in her Footscray Hospital office, O'Connell struggles to answer at first. "Um. I think, to, um, help young people develop a better world," she says. And then to everyone's surprise – especially her own – she begins to cry. "Why am I so emotional about this? I don't understand." We can come back to this, I say. "No. There are so many things young people can do but to create good science, you create a better future." In what way? "Oh well, you know, to improve health is just intrinsically good. To improve relationships between men and women is just intrinsically good."
O'Connell's voice is breaking up. She is genuinely confused about why she's crying. Wilson, the media manager, has tears in her eyes. It's as if we've all suddenly fallen through a hole into a shaky new paradigm. I suspect O'Connell doesn't spend much time reflecting on her motivation; she later says that "navel-gazing is pathological". O'Connell thinks, trying to search for a reason for her tears, then gathers herself. "Anyway, I didn't ask for any of this stuff, it just fell on me." What does she mean by that? "All the anatomy stuff. It just arrived on my doorstep." I don't often disagree with a profile subject in the middle of an interview, but I point out that, actually, she looked at that original anatomy book and knew that one day she'd have to fix it. "Yeah," says O'Connell. "Yeah. Well, maybe the logical conclusion is just to keep on going."
She stands up and reaches for a tissue. Twenty years on from her first ground-breaking paper, there's still more work to do. Some further work on the anatomy of the urethra is next. Her work has raised awareness about preserving sexual sensation in pelvic-area surgery but there's plenty of room for improvement. And she's just been appointed the convenor for an International Continence Society meeting in Melbourne in 2021. "I could have said no," she says. "But if you can do something, why not do it? Most people spend all their time trying to get home to watch the television. For what? Really? You know? People run a mile from doing something, and why? What are you here for? It's ridiculous."
It's almost a month since I first interviewed O'Connell and despite several requests, about which I am starting to feel self-conscious, I still haven't received the G-spot paper. Apparently it was sent, but never arrived in my inbox. And then, finally, I get it.
A sexologist called Beverley Whipple popularised the G-spot, named after Ernst Gräfenberg, a German gynaecologist who first floated the idea in 1950. It's supposed to be a sensitive part on the stomach side of the vaginal wall and, as recently as 2012, American gynaecological surgeon Adam Ostrzenski declared he had found it, calling it a "well-delineated sac" – his scientific journal article was ranked as one of the most popular of that year.
But the G-spot has confounded many who go looking for it and there's a long-running debate about its existence. American bioethicist Jeffrey Spike has said it belonged "in the same category as angels and unicorns". A few years ago, when a journalist asked her whether there really was a G-spot, O'Connell decided she would approach it, as always, scientifically. She and her team dissected the urethra and vaginal wall of 13 cadavers. They reported in a paper published last year that the G-spot "does not exist as an anatomic construct".
So does that mean there's no such thing as a vaginal orgasm? Essentially yes, anatomically speaking, but there's a little more complexity. Basically the vagina itself has no erectile tissue, but any pressure applied can push on the aroused internal clitoris, particularly the bulbs, which are on either side of the lower vaginal wall. "So presumably with intercourse or play," says O'Connell, "there will be movement of all that erectile tissue [around the vaginal wall]. The shape of people's bulbs varies … but there are enough reasons why for some women, vaginal penetration will be associated with orgasm, particularly given the location of erectile tissue around the opening of the vagina."
O'Connell's work echoed that of French gynaecologists Odile Buisson and Pierre Foldès (the latter is famous for reconstructing clitorises for victims of female genital mutilation). Using ultrasound, they did various studies looking at the stimulated clitoris and also the clitoris and vaginal penetration. They even did an ultrasound of a couple having sex. "The G-spot," they noted in a 2009 paper, "could be explained by the richly innervated clitoris."

Sexologist Tanya Koens on the clitoris: “Don’t go straight for the glans and start pressing it like a button!”Credit:James Brickwood
Tanya Koens first came across O'Connell's research 14 years ago, when she was studying to become a sexologist. "I was like, 'Wow. Whoa. Whoa! How come this wasn't taught in school?' " Since then, Koens, who regularly appears on radio station Triple J talking about sex, has immersed herself in genital anatomy. It's her basic starting point with the men and women who see her for sex therapy in her practice in Sydney's Surry Hills. She's even got an anatomically correct, 10-centimetre-long 3D model of the clitoris. "Helen's work has been really amazing," she says. "And I take that theory and wrap it around clinical experience where I see things happening over and over again."
In November, Koens was on a sex therapy study intensive, learning and teaching about sexual anatomy. Late at night, after she returned from leading a "vulva class", she emailed me the advice she gives clients about making the most of the whole, anatomically correct clitoris. She says while it can take some women very little time to orgasm, the senior sexologists she studied under have timed the full engorgement of the whole clitoris at between 45 and 60 minutes.
You've got to treat us like a beautiful old vintage car and warm us up in the garage before you take us out for a drive.
"It's totally possible to have intercourse-style sex before that point – but many people are having that kind of sex too early and it is causing pain and discomfort for a great many folk." She says the clitoris works best with a gentle start-up. "Don't go straight for the glans and start pressing it like a button!" she tells her clients. "Start with kissing, touching the outside of the body and working your way in so that the genitals are getting the idea that they are going to get touched, but you are going to tease us." The clitoral system, she says, can feel nice with pressure on the outside of the vulva, which stimulates the bulbs inside. "Pressure can be applied via thumb pads or heel of hand." The clitoral shaft, just above the glans, can "feel particularly delicious when a small amount of pressure and movement is applied".

Tanya Koens' 10cm-long, anatomically correct, 3D clitoris model.Credit:James Brickwood
She says it's good to understand that with enough arousal, the bulbs swell and push against the walls of the vagina "making it a perfect fit for whatever we put in there, whatever size it is". "I get a lot of men going, 'My girlfriend's got a flabby vagina and I don't like it.' And I say, 'Well, maybe you are not doing your job well of warming up your lovely lady. You've got to treat us like a beautiful old vintage car and warm us up in the garage before you take us out for a drive.'
"I always say that if we treated everyone's arousal system as if it is male – which we have done for a long time – there is going to be a lot of bad sex and sex that is tolerated. If we treat everybody as if they had female arousal systems, everybody is going to have good sex all the time. We just need to slow down and let our bodies do their thing."
Helen O'Connell is not a sex guru. She is not Bettina Arndt or the eccentric sex therapist played by Barbra Streisand in Meet the Fockers. She just knows about the bits. Talking to her about actual sex is a bit like asking the mechanic about what music you should play in your car. But that doesn't stop me trying, of course.
"I get the impression," says O'Connell, over a chicken schnitzel and salad, "that sexual health is a lot about free time." I've arm-twisted her into a quick lunch at the Footscray Hospital cafe and we're discussing the orgasm gap: a 2014 survey by the Australian Study of Health and Relationships found 66 per cent of heterosexual women reported orgasms at their most recent sexual encounter, compared to 92 per cent of men. International research has put the orgasm rate for lesbians as high as 86 per cent. Women, O'Connell says, still carry the bulk of domestic labour and are "not enculturated to chill and relax".
"We are fed all these images of shopping and perfection and 'You've got to get your nails done.' The myriad things that you have to do now to comply with some idea of acceptable beauty is just unbelievable," she says. "And let's face it, men don't have to tick those boxes, they just have to rock up. The barriers for women are just absurd."
It takes me until the last phone call with O'Connell to finally ask the question I know I have to ask. It's a mortifying question to ask such a serious person and top-flight surgeon, but here goes: does it improve one's sex life to be a clitoris guru? I get what's coming to me. "That's really tacky, though, isn't it? It's probably better to not answer that question, Melissa."
Fair enough. But then she tells me about a guy who does research into erectile therapy who injected his penis just before stepping up to the lectern. That's where you would draw the line, I say. "Yeah," O'Connell says. "That's not me."
To read more from Good Weekend magazine, visit our page at The Sydney Morning Herald, The Age and Brisbane Times.
Source: Read Full Article




